
UNITED STATES
SECURITIES AND EXCHANGE COMMISSION
Washington, D.C. 20549
FORM 6-K
REPORT OF FOREIGN PRIVATE ISSUER PURSUANT TO RULE 13a-16 OR 15d-16 UNDER THE SECURITIES EXCHANGE ACT OF 1934
For the month of May, 2026.
Commission File Number: 001-40530
GH Research PLC
(Exact name of registrant as specified in its charter)
Joshua Dawson House
Dawson Street
Dublin 2
D02 RY95
Ireland
(Address of principal executive office)
Indicate by check mark whether the registrant files or will file annual reports under cover of Form 20-F or Form 40-F:
|
Form 20-F
|
☒ |
Form 40-F
|
☐ |
GH Research PLC (the “Company”) will attend the American Society of Clinical Psychopharmacology (“ASCP”) Annual Meeting, which is scheduled to take place from May 26 – 29, 2026, in Miami, Florida (the “Congress”).
The Company will present posters during the Congress as part of Poster Session I.
A copy of the poster to be presented by Roger S. McIntyre is attached hereto as Exhibit 99.1.
A copy of the poster to be presented by Michael E. Thase is attached hereto as Exhibit 99.2.
A copy of the poster to be presented by Wiesław J. Cubała is attached hereto as Exhibit 99.3.
1
Exhibit Index
|
Exhibit No.
|
Description
|
|
Poster presented by Roger S. McIntyre, with Title: Rapid and Sustained Improvement in Anhedonia Following Inhaled Mebufotenin (GH001) Treatment in Patients With Treatment-Resistant Depression
|
|
|
Poster presented by Michael E. Thase, with Title: GH001 Efficacy is Independent of Prior Antidepressant Treatment Failures in Treatment-Resistant Depression: A Post Hoc Analysis of a Phase 2b Randomized
Controlled Trial
|
|
|
Poster presented by Wiesław J. Cubała, with Title: Impact of GH001 on Depressive Symptoms, Anxiety, and Quality of Life in Treatment-Resistant Depression: Results from a Phase 2b Trial
|
2
SIGNATURE
Pursuant to the requirements of the Securities Exchange Act of 1934, the registrant has duly caused this report to be signed on its behalf by the undersigned, thereunto duly authorized.
|
GH Research PLC
|
||
|
Date: May 21, 2026
|
||
|
By:
|
/s/ Julie Ryan
|
|
|
Name:
|
Julie Ryan
|
|
|
Title:
|
Vice President, Finance
|
|
3
Exhibit 99.1
Apparent sadness Reported sadness Concentration difficulty Lassitude Inability to feel Mean (SD) Change
from Baseline in MADRS Anhedonia Factor Items at Day 8 Results Disposition and Baseline Characteristics Disposition and baseline characteristics are presented in Table 1 Mean (SD) total MADRS scores at baseline were 29.0 (5.4) for GH001 and
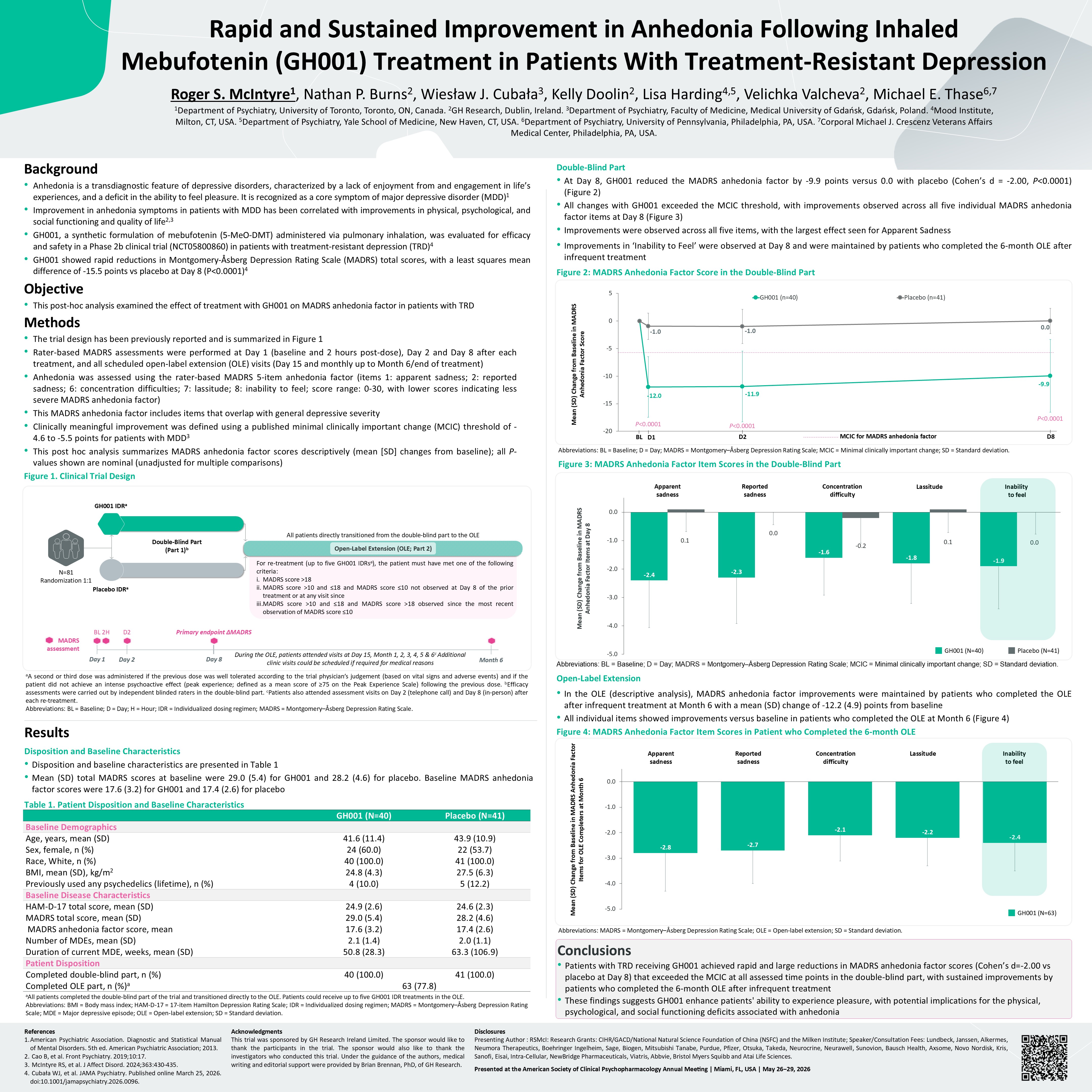
28.2 (4.6) for placebo. Baseline MADRS anhedonia factor scores were 17.6 (3.2) for GH001 and 17.4 (2.6) for placebo Table 1. Patient Disposition and Baseline Characteristics Background Anhedonia is a transdiagnostic feature of depressive
disorders, characterized by a lack of enjoyment from and engagement in life’s experiences, and a deficit in the ability to feel pleasure. It is recognized as a core symptom of major depressive disorder (MDD)1 Improvement in anhedonia symptoms
in patients with MDD has been correlated with improvements in physical, psychological, and social functioning and quality of life2,3 GH001, a synthetic formulation of mebufotenin (5-MeO-DMT) administered via pulmonary inhalation, was evaluated
for efficacy and safety in a Phase 2b clinical trial (NCT05800860) in patients with treatment-resistant depression (TRD)4 GH001 showed rapid reductions in Montgomery-Åsberg Depression Rating Scale (MADRS) total scores, with a least squares
mean difference of -15.5 points vs placebo at Day 8 (P<0.0001)4 Objective This post-hoc analysis examined the effect of treatment with GH001 on MADRS anhedonia factor in patients with TRD Methods The trial design has been previously
reported and is summarized in Figure 1 Rater-based MADRS assessments were performed at Day 1 (baseline and 2 hours post-dose), Day 2 and Day 8 after each treatment, and all scheduled open-label extension (OLE) visits (Day 15 and monthly up to
Month 6/end of treatment) Anhedonia was assessed using the rater-based MADRS 5-item anhedonia factor (items 1: apparent sadness; 2: reported sadness; 6: concentration difficulties; 7: lassitude; 8: inability to feel; score range: 0-30, with
lower scores indicating less severe MADRS anhedonia factor) This MADRS anhedonia factor includes items that overlap with general depressive severity Clinically meaningful improvement was defined using a published minimal clinically important
change (MCIC) threshold of -4.6 to -5.5 points for patients with MDD3 This post hoc analysis summarizes MADRS anhedonia factor scores descriptively (mean [SD] changes from baseline); all P-values shown are nominal (unadjusted for multiple
comparisons) Figure 1. Clinical Trial Design References American Psychiatric Association. Diagnostic and Statistical Manual of Mental Disorders. 5th ed. American Psychiatric Association; 2013. Cao B, et al. Front Psychiatry. 2019;10:17.
McIntyre RS, et al. J Affect Disord. 2024;363:430-435. Cubała WJ, et al. JAMA Psychiatry. Published online March 25, 2026. doi:10.1001/jamapsychiatry.2026.0096. Acknowledgments This trial was sponsored by GH Research Ireland Limited. The
sponsor would like to thank the participants in the trial. The sponsor would also like to thank the investigators who conducted this trial. Under the guidance of the authors, medical writing and editorial support were provided by Brian Brennan,
PhD, of GH Research. Disclosures Presenting Author : RSMcI: Research Grants: CIHR/GACD/National Natural Science Foundation of China (NSFC) and the Milken Institute; Speaker/Consultation Fees: Lundbeck, Janssen, Alkermes, Neumora
Therapeutics, Boehringer Ingelheim, Sage, Biogen, Mitsubishi Tanabe, Purdue, Pfizer, Otsuka, Takeda, Neurocrine, Neurawell, Sunovion, Bausch Health, Axsome, Novo Nordisk, Kris, Sanofi, Eisai, Intra-Cellular, NewBridge Pharmaceuticals, Viatris,
Abbvie, Bristol Myers Squibb and Atai Life Sciences. Presented at the American Society of Clinical Psychopharmacology Annual Meeting | Miami, FL, USA | May 26−29, 2026 Conclusions Patients with TRD receiving GH001 achieved rapid and large
reductions in MADRS anhedonia factor scores (Cohen’s d=-2.00 vs placebo at Day 8) that exceeded the MCIC at all assessed time points in the double-blind part, with sustained improvements by patients who completed the 6-month OLE after
infrequent treatment These findings suggests GH001 enhance patients' ability to experience pleasure, with potential implications for the physical, psychological, and social functioning deficits associated with anhedonia Roger S. McIntyre1,
Nathan P. Burns2, Wiesław J. Cubała3, Kelly Doolin2, Lisa Harding4,5, Velichka Valcheva2, Michael E. Thase6,7 1Department of Psychiatry, University of Toronto, Toronto, ON, Canada. 2GH Research, Dublin, Ireland. 3Department of Psychiatry,
Faculty of Medicine, Medical University of Gdańsk, Gdańsk, Poland. 4Mood Institute, Milton, CT, USA. 5Department of Psychiatry, Yale School of Medicine, New Haven, CT, USA. 6Department of Psychiatry, University of Pennsylvania, Philadelphia,
PA, USA. 7Corporal Michael J. Crescenz Veterans Affairs Medical Center, Philadelphia, PA, USA. Rapid and Sustained Improvement in Anhedonia Following Inhaled Mebufotenin (GH001) Treatment in Patients With Treatment-Resistant Depression aA
second or third dose was administered if the previous dose was well tolerated according to the trial physician’s judgement (based on vital signs and adverse events) and if the patient did not achieve an intense psychoactive effect (peak
experience; defined as a mean score of ≥75 on the Peak Experience Scale) following the previous dose. bEfficacy assessments were carried out by independent blinded raters in the double-blind part. cPatients also attended assessment visits on
Day 2 (telephone call) and Day 8 (in-person) after each re-treatment. Abbreviations: BL = Baseline; D = Day; H = Hour; IDR = Individualized dosing regimen; MADRS = Montgomery–Åsberg Depression Rating Scale. aAll patients completed the
double-blind part of the trial and transitioned directly to the OLE. Patients could receive up to five GH001 IDR treatments in the OLE. Abbreviations: BMI = Body mass index; HAM-D-17 = 17-item Hamilton Depression Rating Scale; IDR =
Individualized dosing regimen; MADRS = Montgomery–Åsberg Depression Rating Scale; MDE = Major depressive episode; OLE = Open-label extension; SD = Standard deviation. Double-Blind Part At Day 8, GH001 reduced the MADRS anhedonia factor by
-9.9 points versus 0.0 with placebo (Cohen’s d = -2.00, P<0.0001) (Figure 2) All changes with GH001 exceeded the MCIC threshold, with improvements observed across all five individual MADRS anhedonia factor items at Day 8 (Figure
3) Improvements were observed across all five items, with the largest effect seen for Apparent Sadness Improvements in ‘Inability to Feel’ were observed at Day 8 and were maintained by patients who completed the 6-month OLE after infrequent
treatment Figure 2: MADRS Anhedonia Factor Score in the Double-Blind Part Abbreviations: BL = Baseline; D = Day; MADRS = Montgomery–Åsberg Depression Rating Scale; MCIC = Minimal clinically important change; SD = Standard deviation. Figure
3: MADRS Anhedonia Factor Item Scores in the Double-Blind Part Abbreviations: BL = Baseline; D = Day; MADRS = Montgomery–Åsberg Depression Rating Scale; MCIC = Minimal clinically important change; SD = Standard deviation. Open-Label
Extension In the OLE (descriptive analysis), MADRS anhedonia factor improvements were maintained by patients who completed the OLE after infrequent treatment at Month 6 with a mean (SD) change of -12.2 (4.9) points from baseline All
individual items showed improvements versus baseline in patients who completed the OLE at Month 6 (Figure 4) Figure 4: MADRS Anhedonia Factor Item Scores in Patient who Completed the 6-month OLE Abbreviations: MADRS = Montgomery–Åsberg
Depression Rating Scale; OLE = Open-label extension; SD = Standard deviation. During the OLE, patients attended visits at Day 15, Month 1, 2, 3, 4, 5 & 6c Additional clinic visits could be scheduled if required for medical reasons For
re-treatment (up to five GH001 IDRsa), the patient must have met one of the following criteria: MADRS score >18 MADRS score >10 and ≤18 and MADRS score ≤10 not observed at Day 8 of the prior treatment or at any visit since MADRS
score >10 and ≤18 and MADRS score >18 observed since the most recent observation of MADRS score ≤10 Open-Label Extension (OLE; Part 2) N=81 Randomization 1:1 Double-Blind Part (Part 1)b All patients directly transitioned from the
double-blind part to the OLE Placebo IDRa GH001 IDRa BL 2H Day 1 Primary endpoint ΔMADRS Day 8 MADRS assessment Month 6 D2 Day 2 GH001 (N=40) Placebo (N=41) Baseline Demographics Age, years, mean (SD) 41.6 (11.4) 43.9
(10.9) Sex, female, n (%) 24 (60.0) 22 (53.7) Race, White, n (%) 40 (100.0) 41 (100.0) BMI, mean (SD), kg/m2 24.8 (4.3) 27.5 (6.3) Previously used any psychedelics (lifetime), n (%) 4 (10.0) 5 (12.2) Baseline Disease
Characteristics HAM-D-17 total score, mean (SD) 24.9 (2.6) 24.6 (2.3) MADRS total score, mean (SD) 29.0 (5.4) 28.2 (4.6) MADRS anhedonia factor score, mean 17.6 (3.2) 17.4 (2.6) Number of MDEs, mean (SD) 2.1 (1.4) 2.0
(1.1) Duration of current MDE, weeks, mean (SD) 50.8 (28.3) 63.3 (106.9) Patient Disposition Completed double-blind part, n (%) 40 (100.0) 41 (100.0) Completed OLE part, n (%)a 63 (77.8) Mean (SD) Change from Baseline in MADRS
Anhedonia Factor Score BL D1 D2 D8 MCIC for MADRS anhedonia factor P<0.0001 P<0.0001 P<0.0001 Apparent sadness Reported sadness Concentration difficulty Lassitude Inability to feel Mean (SD) Change from Baseline in
MADRS Anhedonia Factor Items for OLE Completers at Month 6 GH001 (N=40) Placebo (N=41) GH001 (N=63)
Exhibit 99.2
Remission Rate (MADRS ≤10), % GH001 Day 8 Prior Treatment Failure Remission Rate
(MADRS ≤10), % GH001 EOT/Month 6 Prior Treatment Failure Remission Rate (MADRS ≤10), % STAR*D Reference Progressive Attenuation Results Table 1. Demographics and Baseline Characteristics Background Treatment-resistant depression (TRD)
is associated with persistent symptoms and significant unmet need for effective treatment1 Staging models for TRD have demonstrated that the number of prior treatment failures is among the strongest negative prognostic factors for subsequent
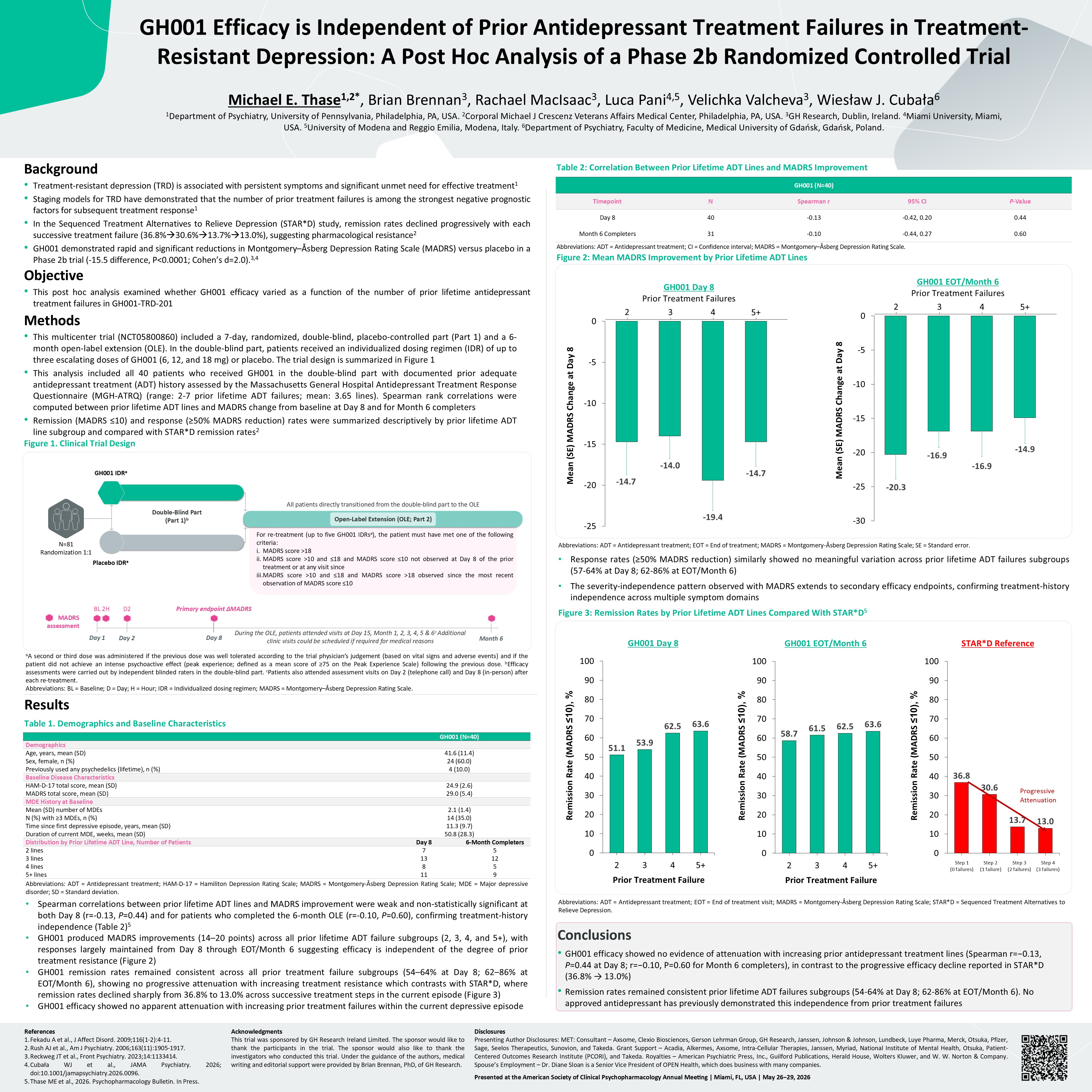
treatment response1 In the Sequenced Treatment Alternatives to Relieve Depression (STAR*D) study, remission rates declined progressively with each successive treatment failure (36.8%30.6%13.7%13.0%), suggesting pharmacological
resistance2 GH001 demonstrated rapid and significant reductions in Montgomery–Åsberg Depression Rating Scale (MADRS) versus placebo in a Phase 2b trial (-15.5 difference, P<0.0001; Cohen’s d=2.0).3,4 Objective This post hoc analysis
examined whether GH001 efficacy varied as a function of the number of prior lifetime antidepressant treatment failures in GH001-TRD-201 Methods This multicenter trial (NCT05800860) included a 7-day, randomized, double-blind,
placebo-controlled part (Part 1) and a 6-month open-label extension (OLE). In the double-blind part, patients received an individualized dosing regimen (IDR) of up to three escalating doses of GH001 (6, 12, and 18 mg) or placebo. The trial
design is summarized in Figure 1 This analysis included all 40 patients who received GH001 in the double-blind part with documented prior adequate antidepressant treatment (ADT) history assessed by the Massachusetts General Hospital
Antidepressant Treatment Response Questionnaire (MGH-ATRQ) (range: 2-7 prior lifetime ADT failures; mean: 3.65 lines). Spearman rank correlations were computed between prior lifetime ADT lines and MADRS change from baseline at Day 8 and for
Month 6 completers Remission (MADRS ≤10) and response (≥50% MADRS reduction) rates were summarized descriptively by prior lifetime ADT line subgroup and compared with STAR*D remission rates2 Figure 1. Clinical Trial Design References Fekadu
A et al., J Affect Disord. 2009;116(1-2):4-11. Rush AJ et al., Am J Psychiatry. 2006;163(11):1905-1917. Reckweg JT et al., Front Psychiatry. 2023;14:1133414. Cubała WJ et al., JAMA Psychiatry. 2026;
doi:10.1001/jamapsychiatry.2026.0096. Thase ME et al., 2026. Psychopharmacology Bulletin. In Press. Acknowledgments This trial was sponsored by GH Research Ireland Limited. The sponsor would like to thank the participants in the trial. The
sponsor would also like to thank the investigators who conducted this trial. Under the guidance of the authors, medical writing and editorial support were provided by Brian Brennan, PhD, of GH Research. Disclosures Presenting Author
Disclosures: MET: Consultant – Axsome, Clexio Biosciences, Gerson Lehrman Group, GH Research, Janssen, Johnson & Johnson, Lundbeck, Luye Pharma, Merck, Otsuka, Pfizer, Sage, Seelos Therapeutics, Sunovion, and Takeda. Grant Support – Acadia,
Alkermes, Axsome, Intra-Cellular Therapies, Janssen, Myriad, National Institute of Mental Health, Otsuka, Patient-Centered Outcomes Research Institute (PCORI), and Takeda. Royalties – American Psychiatric Press, Inc., Guilford Publications,
Herald House, Wolters Kluwer, and W. W. Norton & Company. Spouse’s Employment – Dr. Diane Sloan is a Senior Vice President of OPEN Health, which does business with many companies. Presented at the American Society of Clinical
Psychopharmacology Annual Meeting | Miami, FL, USA | May 26−29, 2026 Conclusions GH001 efficacy showed no evidence of attenuation with increasing prior antidepressant treatment lines (Spearman r=−0.13, P=0.44 at Day 8; r=−0.10, P=0.60 for
Month 6 completers), in contrast to the progressive efficacy decline reported in STAR*D (36.8% → 13.0%) Remission rates remained consistent prior lifetime ADT failures subgroups (54-64% at Day 8; 62-86% at EOT/Month 6). No approved
antidepressant has previously demonstrated this independence from prior treatment failures Michael E. Thase1,2*, Brian Brennan3, Rachael MacIsaac3, Luca Pani4,5, Velichka Valcheva3, Wiesław J. Cubała6 1Department of Psychiatry, University of
Pennsylvania, Philadelphia, PA, USA. 2Corporal Michael J Crescenz Veterans Affairs Medical Center, Philadelphia, PA, USA. 3GH Research, Dublin, Ireland. 4Miami University, Miami, USA. 5University of Modena and Reggio Emilia, Modena, Italy.
6Department of Psychiatry, Faculty of Medicine, Medical University of Gdańsk, Gdańsk, Poland. GH001 Efficacy is Independent of Prior Antidepressant Treatment Failures in Treatment-Resistant Depression: A Post Hoc Analysis of a Phase 2b
Randomized Controlled Trial aA second or third dose was administered if the previous dose was well tolerated according to the trial physician’s judgement (based on vital signs and adverse events) and if the patient did not achieve an intense
psychoactive effect (peak experience; defined as a mean score of ≥75 on the Peak Experience Scale) following the previous dose. bEfficacy assessments were carried out by independent blinded raters in the double-blind part. cPatients also
attended assessment visits on Day 2 (telephone call) and Day 8 (in-person) after each re-treatment. Abbreviations: BL = Baseline; D = Day; H = Hour; IDR = Individualized dosing regimen; MADRS = Montgomery–Åsberg Depression Rating Scale.
Abbreviations: ADT = Antidepressant treatment; HAM-D-17 = Hamiliton Depression Rating Scale; MADRS = Montgomery-Åsberg Depression Rating Scale; MDE = Major depressive disorder; SD = Standard deviation. Spearman correlations between prior
lifetime ADT lines and MADRS improvement were weak and non-statistically significant at both Day 8 (r=-0.13, P=0.44) and for patients who completed the 6-month OLE (r=-0.10, P=0.60), confirming treatment-history independence (Table 2)5 GH001
produced MADRS improvements (14–20 points) across all prior lifetime ADT failure subgroups (2, 3, 4, and 5+), with responses largely maintained from Day 8 through EOT/Month 6 suggesting efficacy is independent of the degree of prior treatment
resistance (Figure 2) GH001 remission rates remained consistent across all prior treatment failure subgroups (54–64% at Day 8; 62–86% at EOT/Month 6), showing no progressive attenuation with increasing treatment resistance which contrasts with
STAR*D, where remission rates declined sharply from 36.8% to 13.0% across successive treatment steps in the current episode (Figure 3) GH001 efficacy showed no apparent attenuation with increasing prior treatment failures within the current
depressive episode Table 2: Correlation Between Prior Lifetime ADT Lines and MADRS Improvement Abbreviations: ADT = Antidepressant treatment; EOT = End of treatment; MADRS = Montgomery-Åsberg Depression Rating Scale; SE = Standard
error. Response rates (≥50% MADRS reduction) similarly showed no meaningful variation across prior lifetime ADT failures subgroups (57-64% at Day 8; 62-86% at EOT/Month 6) The severity-independence pattern observed with MADRS extends to
secondary efficacy endpoints, confirming treatment-history independence across multiple symptom domains Figure 3: Remission Rates by Prior Lifetime ADT Lines Compared With STAR*D5 Abbreviations: ADT = Antidepressant treatment; EOT = End of
treatment visit; MADRS = Montgomery-Åsberg Depression Rating Scale; STAR*D = Sequenced Treatment Alternatives to Relieve Depression. During the OLE, patients attended visits at Day 15, Month 1, 2, 3, 4, 5 & 6c Additional clinic visits
could be scheduled if required for medical reasons For re-treatment (up to five GH001 IDRsa), the patient must have met one of the following criteria: MADRS score >18 MADRS score >10 and ≤18 and MADRS score ≤10 not observed at Day 8
of the prior treatment or at any visit since MADRS score >10 and ≤18 and MADRS score >18 observed since the most recent observation of MADRS score ≤10 Open-Label Extension (OLE; Part 2) N=81 Randomization 1:1 Double-Blind Part (Part
1)b All patients directly transitioned from the double-blind part to the OLE Placebo IDRa GH001 IDRa BL 2H Day 1 Primary endpoint ΔMADRS Day 8 MADRS assessment Month 6 D2 Day 2 GH001 (N=40) Demographics Age, years, mean
(SD) 41.6 (11.4) Sex, female, n (%) 24 (60.0) Previously used any psychedelics (lifetime), n (%) 4 (10.0) Baseline Disease Characteristics HAM-D-17 total score, mean (SD) 24.9 (2.6) MADRS total score, mean (SD) 29.0 (5.4) MDE History
at Baseline Mean (SD) number of MDEs 2.1 (1.4) N (%) with ≥3 MDEs, n (%) 14 (35.0) Time since first depressive episode, years, mean (SD) 11.3 (9.7) Duration of current MDE, weeks, mean (SD) 50.8 (28.3) Distribution by Prior Lifetime
ADT Line, Number of Patients Day 8 6-Month Completers 2 lines 7 5 3 lines 13 12 4 lines 8 5 5+ lines 11 9 Mean (SE) MADRS Change at Day 8 GH001 Day 8 Prior Treatment Failures 2 3 4 5+ Mean (SE) MADRS Change at Day 8 GH001
EOT/Month 6 Prior Treatment Failures 2 3 4 5+ GH001 (N=40) Timepoint N Spearman r 95% CI P-Value Day 8 40 -0.13 -0.42, 0.20 0.44 Month 6 Completers 31 -0.10 -0.44, 0.27 0.60 Step 1 (0 failures) Step 2 (1 failure) Step
3 (2 failures) Step 4 (3 failures) Abbreviations: ADT = Antidepressant treatment; CI = Confidence interval; MADRS = Montgomery–Åsberg Depression Rating Scale. Figure 2: Mean MADRS Improvement by Prior Lifetime ADT Lines
Exhibit 99.3
Abbreviations: LS = Least squares; SE = Standard error; Q-LES-Q-SF = Quality of Life,
Enjoyment, and Satisfaction Questionnaire-Short Form. Table 2: Mean Change from Baseline in Secondary Efficacy Endpoints for Patients who Completed the 6-Month Open-Label Extension (N=63) GH001 (N=37) Placebo (N=40) Results Demographics
and baseline characteristics are presented in Table 1 Table 1. Patient Disposition and Baseline Characteristics Background Treatment-resistant depression (TRD) is associated with persistent symptoms of depression, anxiety, and reduced
quality of life, despite a limited number of treatments being available1-3 Patients with TRD frequently report greater anxiety burden and poorer health-related quality of life compared with patients with treatment-responsive depression,
underscoring the need for treatments that address these domains1-3 GH001, a synthetic formulation of mebufotenin (5-MeO-DMT) administered via pulmonary inhalation, was evaluated for efficacy and safety in a Phase 2b clinical trial
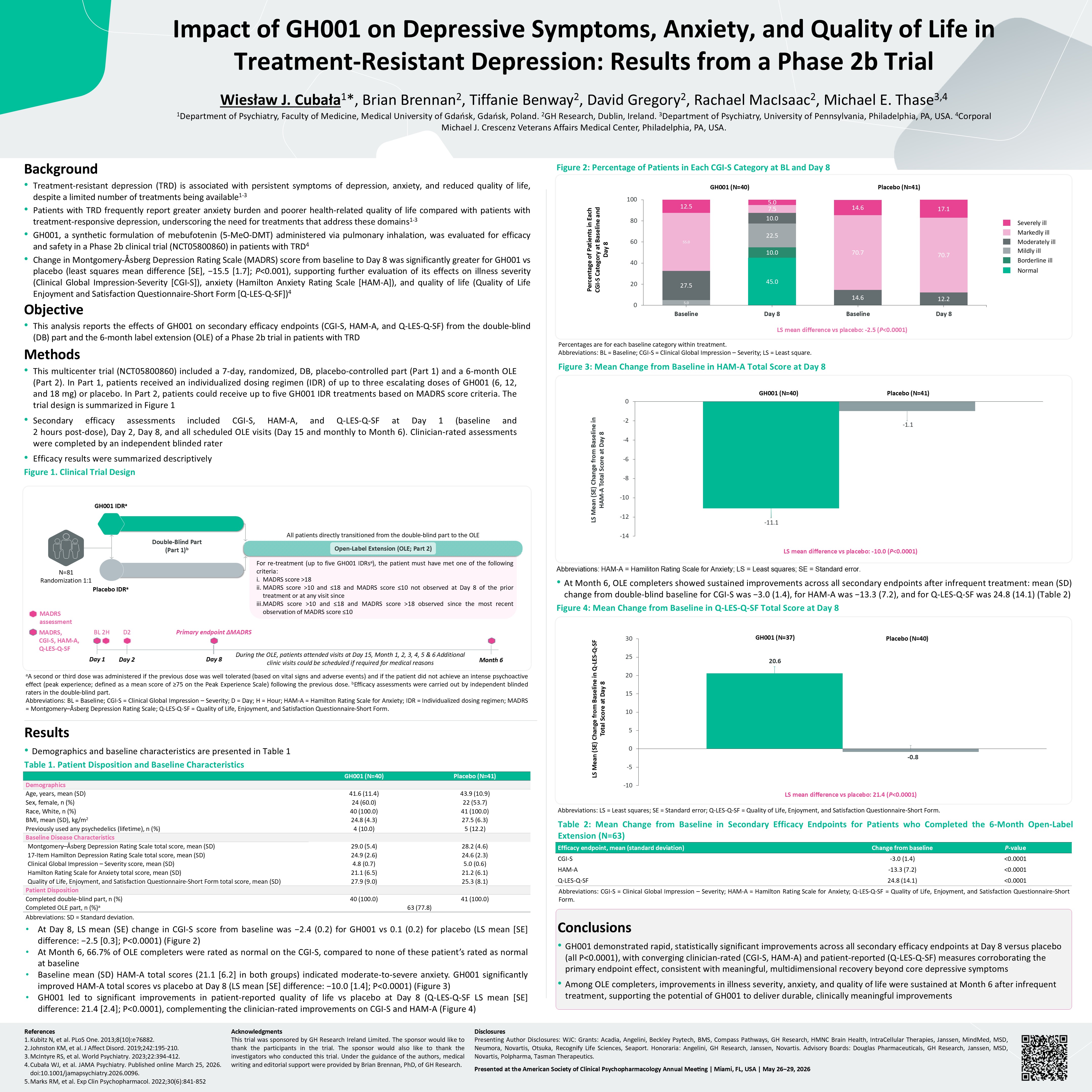
(NCT05800860) in patients with TRD4 Change in Montgomery-Åsberg Depression Rating Scale (MADRS) score from baseline to Day 8 was significantly greater for GH001 vs placebo (least squares mean difference [SE], −15.5 [1.7]; P<0.001),
supporting further evaluation of its effects on illness severity (Clinical Global Impression-Severity [CGI-S]), anxiety (Hamilton Anxiety Rating Scale [HAM-A]), and quality of life (Quality of Life Enjoyment and Satisfaction Questionnaire-Short
Form [Q-LES-Q-SF])4 Objective This analysis reports the effects of GH001 on secondary efficacy endpoints (CGI-S, HAM-A, and Q-LES-Q-SF) from the double-blind (DB) part and the 6-month label extension (OLE) of a Phase 2b trial in patients with
TRD Methods This multicenter trial (NCT05800860) included a 7-day, randomized, DB, placebo-controlled part (Part 1) and a 6-month OLE (Part 2). In Part 1, patients received an individualized dosing regimen (IDR) of up to three escalating
doses of GH001 (6, 12, and 18 mg) or placebo. In Part 2, patients could receive up to five GH001 IDR treatments based on MADRS score criteria. The trial design is summarized in Figure 1 Secondary efficacy assessments included CGI-S, HAM-A, and
Q-LES-Q-SF at Day 1 (baseline and 2 hours post-dose), Day 2, Day 8, and all scheduled OLE visits (Day 15 and monthly to Month 6). Clinician-rated assessments were completed by an independent blinded rater Efficacy results were summarized
descriptively Figure 1. Clinical Trial Design References Kubitz N, et al. PLoS One. 2013;8(10):e76882. Johnston KM, et al. J Affect Disord. 2019;242:195-210. McIntyre RS, et al. World Psychiatry. 2023;22:394-412. Cubała WJ, et al. JAMA
Psychiatry. Published online March 25, 2026. doi:10.1001/jamapsychiatry.2026.0096. Marks RM, et al. Exp Clin Psychopharmacol. 2022;30(6):841-852 Acknowledgments This trial was sponsored by GH Research Ireland Limited. The sponsor would like
to thank the participants in the trial. The sponsor would also like to thank the investigators who conducted this trial. Under the guidance of the authors, medical writing and editorial support were provided by Brian Brennan, PhD, of GH
Research. Disclosures Presenting Author Disclosures: WJC: Grants: Acadia, Angelini, Beckley Psytech, BMS, Compass Pathways, GH Research, HMNC Brain Health, IntraCellular Therapies, Janssen, MindMed, MSD, Neumora, Novartis, Otsuka, Recognify
Life Sciences, Seaport. Honoraria: Angelini, GH Research, Janssen, Novartis. Advisory Boards: Douglas Pharmaceuticals, GH Research, Janssen, MSD, Novartis, Polpharma, Tasman Therapeutics. Presented at the American Society of Clinical
Psychopharmacology Annual Meeting | Miami, FL, USA | May 26−29, 2026 Conclusions GH001 demonstrated rapid, statistically significant improvements across all secondary efficacy endpoints at Day 8 versus placebo (all P<0.0001), with
converging clinician-rated (CGI-S, HAM-A) and patient-reported (Q-LES-Q-SF) measures corroborating the primary endpoint effect, consistent with meaningful, multidimensional recovery beyond core depressive symptoms Among OLE completers,
improvements in illness severity, anxiety, and quality of life were sustained at Month 6 after infrequent treatment, supporting the potential of GH001 to deliver durable, clinically meaningful improvements Wiesław J. Cubała1*, Brian Brennan2,
Tiffanie Benway2, David Gregory2, Rachael MacIsaac2, Michael E. Thase3,4 1Department of Psychiatry, Faculty of Medicine, Medical University of Gdańsk, Gdańsk, Poland. 2GH Research, Dublin, Ireland. 3Department of Psychiatry, University of
Pennsylvania, Philadelphia, PA, USA. 4Corporal Michael J. Crescenz Veterans Affairs Medical Center, Philadelphia, PA, USA. Impact of GH001 on Depressive Symptoms, Anxiety, and Quality of Life in Treatment-Resistant Depression: Results from a
Phase 2b Trial aA second or third dose was administered if the previous dose was well tolerated (based on vital signs and adverse events) and if the patient did not achieve an intense psychoactive effect (peak experience; defined as a mean
score of ≥75 on the Peak Experience Scale) following the previous dose. bEfficacy assessments were carried out by independent blinded raters in the double-blind part. Abbreviations: BL = Baseline; CGI-S = Clinical Global Impression –
Severity; D = Day; H = Hour; HAM-A = Hamilton Rating Scale for Anxiety; IDR = Individualized dosing regimen; MADRS = Montgomery–Åsberg Depression Rating Scale; Q-LES-Q-SF = Quality of Life, Enjoyment, and Satisfaction Questionnaire-Short Form.
Abbreviations: SD = Standard deviation. At Day 8, LS mean (SE) change in CGI-S score from baseline was −2.4 (0.2) for GH001 vs 0.1 (0.2) for placebo (LS mean [SE] difference: −2.5 [0.3]; P<0.0001) (Figure 2) At Month 6, 66.7% of OLE
completers were rated as normal on the CGI-S, compared to none of these patient’s rated as normal at baseline Baseline mean (SD) HAM-A total scores (21.1 [6.2] in both groups) indicated moderate-to-severe anxiety. GH001 significantly improved
HAM-A total scores vs placebo at Day 8 (LS mean [SE] difference: −10.0 [1.4]; P<0.0001) (Figure 3) GH001 led to significant improvements in patient-reported quality of life vs placebo at Day 8 (Q-LES-Q-SF LS mean [SE] difference: 21.4
[2.4]; P<0.0001), complementing the clinician-rated improvements on CGI-S and HAM-A (Figure 4) Figure 2: Percentage of Patients in Each CGI-S Category at BL and Day 8 Percentages are for each baseline category within treatment.
Abbreviations: BL = Baseline; CGI-S = Clinical Global Impression – Severity; LS = Least square. Figure 3: Mean Change from Baseline in HAM-A Total Score at Day 8 Abbreviations: HAM-A = Hamiliton Rating Scale for Anxiety; LS = Least squares;
SE = Standard error. At Month 6, OLE completers showed sustained improvements across all secondary endpoints after infrequent treatment: mean (SD) change from double-blind baseline for CGI-S was −3.0 (1.4), for HAM-A was −13.3 (7.2), and for
Q-LES-Q-SF was 24.8 (14.1) (Table 2) Figure 4: Mean Change from Baseline in Q-LES-Q-SF Total Score at Day 8 During the OLE, patients attended visits at Day 15, Month 1, 2, 3, 4, 5 & 6 Additional clinic visits could be scheduled if
required for medical reasons For re-treatment (up to five GH001 IDRsa), the patient must have met one of the following criteria: MADRS score >18 MADRS score >10 and ≤18 and MADRS score ≤10 not observed at Day 8 of the prior treatment
or at any visit since MADRS score >10 and ≤18 and MADRS score >18 observed since the most recent observation of MADRS score ≤10 Open-Label Extension (OLE; Part 2) N=81 Randomization 1:1 Double-Blind Part (Part 1)b All patients
directly transitioned from the double-blind part to the OLE Placebo IDRa GH001 IDRa BL 2H Day 1 Primary endpoint ΔMADRS Day 8 MADRS assessment Month 6 D2 Day 2 MADRS, CGI-S, HAM-A, Q-LES-Q-SF GH001 (N=40) Placebo
(N=41) Demographics Age, years, mean (SD) 41.6 (11.4) 43.9 (10.9) Sex, female, n (%) 24 (60.0) 22 (53.7) Race, White, n (%) 40 (100.0) 41 (100.0) BMI, mean (SD), kg/m2 24.8 (4.3) 27.5 (6.3) Previously used any psychedelics
(lifetime), n (%) 4 (10.0) 5 (12.2) Baseline Disease Characteristics Montgomery–Åsberg Depression Rating Scale total score, mean (SD) 29.0 (5.4) 28.2 (4.6) 17-Item Hamilton Depression Rating Scale total score, mean (SD) 24.9 (2.6) 24.6
(2.3) Clinical Global Impression – Severity score, mean (SD) 4.8 (0.7) 5.0 (0.6) Hamilton Rating Scale for Anxiety total score, mean (SD) 21.1 (6.5) 21.2 (6.1) Quality of Life, Enjoyment, and Satisfaction Questionnaire-Short Form total
score, mean (SD) 27.9 (9.0) 25.3 (8.1) Patient Disposition Completed double-blind part, n (%) 40 (100.0) 41 (100.0) Completed OLE part, n (%)a 63 (77.8) Percentage of Patients in Each CGI-S Category at Baseline and Day 8 LS mean
difference vs placebo: -2.5 (P<0.0001) GH001 (N=40) Placebo (N=41) Normal Borderline ill Mildly ill Moderately ill Markedly ill Severely ill LS mean difference vs placebo: -10.0 (P<0.0001) GH001 (N=40) Placebo (N=41) LS Mean
(SE) Change from Baseline in HAM-A Total Score at Day 8 LS mean difference vs placebo: 21.4 (P<0.0001) LS Mean (SE) Change from Baseline in Q-LES-Q-SF Total Score at Day 8 Efficacy endpoint, mean (standard deviation) Change from
baseline P-value CGI-S -3.0 (1.4) <0.0001 HAM-A -13.3 (7.2) <0.0001 Q-LES-Q-SF 24.8 (14.1) <0.0001 Abbreviations: CGI-S = Clinical Global Impression – Severity; HAM-A = Hamilton Rating Scale for Anxiety; Q-LES-Q-SF = Quality
of Life, Enjoyment, and Satisfaction Questionnaire-Short Form.